COVID-19: Hungary reports weekly growth in new cases


The table below includes the number of new COVID-19 infections, coronavirus-related deaths, and the number of infected people in hospital and on ventilator for the week up to 13 September, as well as the week-on-week changes for the past four weeks. (The green cells show the biggest w/w decline (good), while the red/yellow cells show the biggest w/w growth / smallest drop (bad) of the last four weeks.)

Let's see a few charts about the key indicators:


Reading the graphs is somewhat difficult not just because the 16 August report contained apparently false data which did not fit into the trend at all, but also because some figures contradict each other and perhaps logic, as well.
The 23 Aug column above contains three red and one yellow cell because the changes came after impossibly low figures reported a week earlier.
Focus on omicron - studies
Now, a few things worth knowing about the omicron variant and its latest subvariants, BA.4 and BA.5:
- For most people, at least those who are up to date on their Covid vaccinations, the original type of the omicron variant caused a milder illness that resembled the common cold, another form of the coronavirus.
- Anecdotally, doctors say, the symptoms of the BA.4 and BA.5 subvariants are mostly similar to those of the earlier version of the variant.
- Typical symptoms of the omicron subvariants include: sore throat, hoarse voice, cough, fatigue, nasal congestion, runny nose, headache, muscle aches.
- If you are vaccinated, particularly if you’ve had a booster, omicron tends to produce milder infections. For vaccinated people that received no booster(s), typical symptoms include more coughing, more fever and more fatigue.
- There has been evidence that the omicron variant tends not to burrow deeply into the lungs as much as previous variants, but it can replicate faster higher up in the respiratory tract. (In that way, it may act more like bronchitis than pneumonia, causing shortness of breath, coughs and the production of sputum.)
- The time it takes for an infected person to develop symptoms after an exposure may be as little as three days or less, according to the CDC. The incubation period could vary greatly, though, depending on age, underlying health problems and vaccination status.
- In general, symptoms appear to be shorter and milder in the vaccinated compared to the unvaccinated who are more likely to go to the ICU. For the vaccinated, emergency room or hospital stays are also typically shorter with the omicron variant.
- Anyone who has been in contact with an infected person should get tested about 72 hours after the exposure. The CDC recommends testing at least five days after exposure.
- In a , British researchers found that the omicron variant is less likely to cause long Covid symptoms than delta, although all of the 41,361 adult participants who regularly reported their Covid symptoms on a phone app had been vaccinated.
- The best protection against coronavirus, and particularly against BA.4 and BA.5 is to get vaccinated and boosted, as these are easier to catch than the other viruses.
Between June 1, 2021, and Jan 17, 2022, researchers identified 63,002 participants who tested positive for SARS-CoV-2 and reported symptoms in the ZOE COVID app (previously known as the COVID Symptoms Study App).
They found that the prevalence of symptoms that characterise an omicron infection differs from those of the delta SARS-CoV-2 variant,
apparently with less involvement of the lower respiratory tract and reduced probability of hospital admission, [...] a shorter period of illness and potentially of infectiousness.
They found that participants who had received two or three vaccine doses had a lower risk of hospitalisation during omicron prevalence than during delta prevalence. The duration of acute symptoms was also shorter. The researchers found that odds of hospitalisation are 25% lower for omicron than for delta.
They did admit to some study limitations, including the fact that (i) most study participants were vaccinated, (ii) some participants might be more likely to report symptoms than others, and participants using the app were a self-selected group and not representative of the general population, (iii) their populations were matched for age, vaccination status, and sex but not for any other potential confounders, (iv) they were unable to assess the role of previous infection on clinical presentation due to insufficient sample size, (v) they could not match for time elapsed since vaccination.
Another study looked into the infectious viral load (VL) in unvaccinated and vaccinated individuals infected with ancestral, Delta or Omicron SARS-CoV-2.
In this study, they quantified infectious VL in individuals infected with SARS-CoV-2 during the first five symptomatic days by in vitro culturability assay in unvaccinated or vaccinated individuals infected with pre-variant of concern (pre-VOC) SARS-CoV-2, Delta or Omicron BA.1.
Main findings:
- Unvaccinated individuals infected with pre-VOC SARS-CoV-2 had lower infectious VL than Delta-infected unvaccinated individuals.
- Full vaccination (defined as >2 weeks after receipt of the second dose during the primary vaccination series) significantly reduced infectious VL for Delta breakthrough cases compared to unvaccinated individuals.
- For Omicron BA.1 breakthrough cases, reduced infectious VL was observed only in boosted but not in fully vaccinated individuals compared to unvaccinated individuals.
- In addition, infectious VL was lower in fully vaccinated Omicron BA.1-infected individuals compared to fully vaccinated Delta-infected individuals, suggesting that mechanisms other than increased infectious VL contribute to the high infectiousness of SARS-CoV-2 Omicron BA.1.
Our findings indicate that vaccines may lower transmission risk and, therefore, have a public health benefit beyond the individual protection from severe disease.
Overall, they have found that:
- There's a low correlation between genome copies and infectious VL
- Delta-infected unvaccinated individuals have higher infectious VL
- Fully vaccinated individuals have lower infectious VL in Delta-infected individuals
- Booster vaccination leads to lower infectious VL in Omicron-infected individuals
Weekly changes in Hungary
It's worth putting the weekly changes side by side. Note that the reliability of the data is extremely low, but these are the figures we have to work with. Apart from the mid-August fluke the data are consistent.
On the left-hand graph you can see that there is a correlation between the number of new cases, hospital admissions, Covid patients on ventilator and coronavirus-related deaths. For instance, when the number of hospitalisations rose sharply (early July, late July) fatalities also showed an increase with a 7-day lag. The changes in hospitalisations and ventilation have been moving more or less in tandem.
The correlation between rising ventilation figures and deaths (r-h chart) is also apparent, and without the mid-Aug error in the reported figures the pattern of the curves should be more alike. Theoretically, we should see a drop / rise in the light blue curve followed by a similar change in the lilac curve (as in early July) all the way.

Vaccination uptake dwindles further
A total of 3,079 COVID-19 shots have been administered in Hungary over the past seven days, down from 4,168 a week earlier and 5,440 two week earlier.

The daily average dropped 26% to just 440 doses per day.
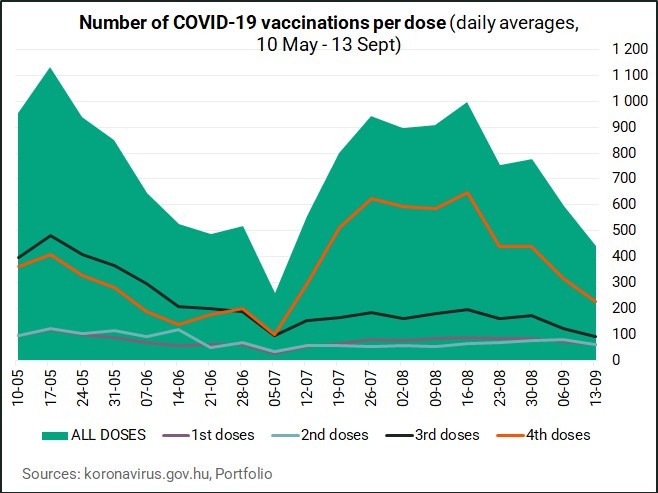

Here's a breakdown of the various doses administered:


The number of Hungarians with SARS-CoV-2 infection in quarantine went up to 3,167 from 2,371 in a week (further up from 1,641 two weeks ago). Not that this means anything amid the current Covid regulations...

Cover photo: Getty Images







